With one paper published today, we published a series of 4 papers on the epidemiology of the pandemic examining what everyone has been generally believing. There are some expected but many surprising outcomes. This is what the four papers summarily say
Much before vaccines came in, the virus had already started losing its virulence rapidly, that continued despite some temporary hick ups. Today it is not much different than flue or common cold. After examining several alternative reasons for this trend we showed that largely evolution of the virus has led to loss of virulence. Vaccines played only a marginal role in this.
Lockdowns and other restrictions were not at all effective in controlling the rate of transmission in the long run.
Small increments in immunity because of subclinical infections and exposure to frequent but small doses of the virus played a major role in shaping the epidemics. All waves were substantially dwarfed than what all models predicted. This was not because of lockdowns, it was because of the small immunity increments conferred by the frequent small exposures. Carefully comparing the testable predictions of the two possible causes unanimously support the small immunity effects model and reject the lockdown model.
The repeated waves were not caused by new variants as most commonly believed. Forget about causation, there is not even statistically significant association of new variants with new waves. The repeated surges were caused by rapidly declining immunity. At times a new variant successfully rode an upcoming wave. It was a consequence, not the cause.
The succession of variants was not mutation limited. The pattern shows clear signs of selection limited evolution.
Links to the four publications showing the above are here
In addition to the published work, there was more analysis and more inferences that remained unpublished, but some of them were presented in a couple of meetings. There is much more in the data that can be explored with new questions. This can be good exercise for students learning public health or statistics or simply learning science. I will illustrate this with a couple of examples below.
The graph shows the appearance and invasion by successive variants in UK, each variant in the proportion of samples sequenced being shown by a different color. The lower half shows the incidence surges, on a date matched scale. By the fundamental principles of statistics one should start with the null hypothesis that emergence of a new variant and the waves of transmission are independent of each other. Because there are so many variants coming up, a new wave may coincide with some upcoming variant by chance alone. Unless this null hypothesis is rejected, one cannot conclude that a wave is associated with a particular variant. This can be done for all countries where there is sufficient variant data. Believe me, this exercise has never been done in published literature. The conclusion that new variants cause a wave was reached just like that, without the minimum required statistical analysis. This is still untapped and open to be analyzed by someone.
Figure 1: The succession of variants each shown in a different color and successive waves of epidemic. What null hypothesis will be appropriate to show significant association of a wave with a variant?
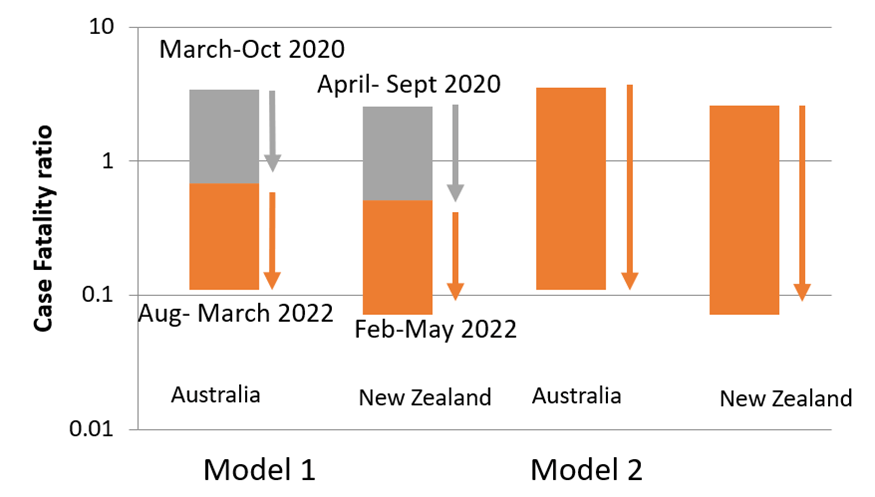
See another example. Was the vaccine responsible for making the infection mild? This question is difficult to answer because of natural immunity being the confounding factor. But Australia and New Zealand offer an opportunity. After an initial surge, these two island countries were successful in keeping free of infection for almost a whole year. Then the infection re-entered and spread widely. But by this time vaccines had reached. About 80 % population got vaccinated and saturated there for multiple reasons. It did not climb to 100%. The mortality in the first wave of March to Sept 2020 was 30 to 35 times higher than that during Aug to March 2022. Because there was practically no natural infection for about one year and immunity is now known to be short lived, we can assume little natural immunity in this population at the beginning of the second wave. Did vaccine cause the 30-35 fold difference? This is impossible because only 80% population was vaccinated. If we go by a limiting assumption 1 (model 1 in the figure) that vaccination completely eliminated mortality in the vaccinated but did not prevent infection, then only a 5 fold difference is expected because 1/5th population remained unvaccinated. The remaining 6-7 fold is not explained by vaccine. If we make the other extreme limiting assumption (Model 2) that the vaccine prevented infection with 100 % efficiency and only the unvaccinated got infected in the second wave, then mortality among the infected shouldn’t have reduced at all, if vaccine was the cause of decreased mortality. The reality should lie somewhere between the two limiting assumptions. This means vaccines explain somewhere between zero and 5 fold difference out of the 30-35 fold difference.
Figure 2: The difference between CFR in the first wave and second wave on a log scale. Gray represents the maximum difference explained by vaccines in models 1 and 2 respectively. The rest is likely to be explained by virus evolution.
I wonder why nobody sees such patterns, nobody challenges the religious like beliefs in the field of public health. This must be because we never teach science as a way to test, examine or challenge a hypothesis. We teach science as a religion.
There are more questions that can be asked with the available data and anyone can do this. I recently announced on my social media accounts that I would welcome any one to join me in addressing many such questions. No qualification requirements other than genuine interest. I received an amazing response. So much that I have to rethink about how to handle this. But I am sure, if I can motivate at least a handful of them so much useful science can be done and so many beliefs re-examined, not only in the pandemic data but in so many other problems of the society that need attention.
Not getting anyone agreeing to review is a growing concern of journal editors. Often editors have to send requests to 10-20 potential reviewers so that one or two agree; keeping the time commitment, the repeated reminders required apart. Editors therefore have a tough job. They make it easy partly by making the invitation and reminder process automated. But that doesn’t address the root cause of the problem.
We had an interesting experience over the last couple of years. For one of our papers, three journals one after the other, took substantial time each with no progress shown on the online updates. After substantial delay, (6 months in one case) they returned the MS saying that they did not find any editor/reviewer agreeing to handle/review the MS. The 6 month delay case was with PLOS One which actually has a large network of editors and reviewers from different fields. I am sure they tried their best to find an appropriate person to agree, but with no result. This is just one example. Experiences across the board show that the problem of not getting reviewers is genuine and widespread.
Then something unexpected (not unexpected for me though!!) happened to our paper. After spending almost two years, trying out many journals and not getting a single review, we decided to publish it in the open peer review journal Qeios. The journal has an AI system to send requests to reviewers in the field. In addition, any reader is welcome to post comments. All comments get publicly posted immediately. The author responses and revisions are also open in the public domain. On posting the paper on this platform something miraculous happened. Reviews started flowing in within a couple of weeks. Today after about 7 weeks, there are 16 reviews received. I just completed replying the reviewers and posting a revised MS. This response contrasts the prior experience of not getting a single review in two years in multiple journals in the prevalent system of confidential peer reviews. So the contrast is between zero reviews in two years versus 16 reviews in 7 weeks.
How does the quality of reviews compare? No comparison specific to this paper is possible because there was no review in the traditional system. A systematic comparative analysis across the two systems with sufficient sample size is not possible unless some of the traditional journals make their reviews public. The traditional journals just want to avoid getting exposed so they will never do this. So I can only talk anecdotally. In my experience with prior publications, there is no difference between the two in the average quality of reviews. On an average both are equally bad. A minority of reviews are really thoughtful, rigorous, appreciating and critical on appropriate issues and therefore useful to improve the quality of the paper. For the reviews on this paper I would say a greater proportion of reviews turned out to be insightful and useful for revision. But there were poor quality reviews as well. Here is the link to the revised paper, all the reviews and replies (https://www.qeios.com/read/GL52DB.2). Readers are welcome to make their own opinion.
Talking about my sample size of a few hundred reviews, majority of reviews have been very superficial, saying nothing critically about the central content and making a few suggestions like improving figure 3b or making the introduction more concise. Some comments such as more clarity is needed are universally true and therefore completely useless unless some specifics are pointed out. A comment about language correction is so common. When the author names sound non-British, a suggestion to get the manuscript refined by a native English speaker has to be there. I tried taking help from professional language service and even after that this comment had to be there. Some reviews are entirely stupid and irresponsible. Precisely this entire range is seen in the reviews received in open peer review system. But the proportion of sensible reviews appears to be slightly greater in open peer review system.
Why is it that conventional journals found it impossible to get reviewers and for the same paper open peer review system had so many reviews in a short time? I can see two distinct but interdependent reasons. One is the accept reject dichotomy. Any kind of debate, differences of opinions and suggestions are useful and important for science. But a reject decision stops this process. The accept-reject dichotomy has actually defeated the purpose of peer reviews. The Qeios system takes this dichotomy away. One of the beliefs behind confidential peer reviews has been that by being anonymous reviewers can avoid the rage from authors and the resultant personal bitterness. The scientific community actually welcomes debates of any kind. They are irked by rejection which takes away the opportunity to debate. Here the authors are always given the freedom to respond and therefore reviews do not end up irritating the authors despite critical comments. Reviewers are not afraid of spoiling the relations and a healthy debate is possible. I suspect that if the social fear is taken off, reviewers actually like to publish the comments with their identity disclosed. The second factor contributing to reviewers’ willingness is that they get a credit for their review and a feeling of participating in the refinement of the paper and thereby progress of the field. This is the true and healthy motivating factor. Other suggestions such as paying the reviewers are unlikely to have the same motivational effect. Reviewers actually seem to like the idea of their comments getting published. This I think is the reason why we received 16 reviews for a paper that did not get a single reviewer in confidential review system.
A promising inference coming from this experience is that there is a simple solution to the problem of reluctance of reviewers and that is to remove confidentiality, discourage anonymity and make the peer reviews public. If accept reject decisions are necessary at all, let a discussion between the editor and authors decide it. Reviewers need not give any accept-reject recommendation. They only write their critical views. If the reviews expose fundamental flaws in the manuscript, authors themselves would like to either remove them or withdraw. If they don’t, their reputation suffers because the flaws pointed out by the reviewers also get published along with the paper.
All this can work only with the assumption that there are readers that actually read the papers and the comments as well. About this I am not so sure or hopeful. The culture of making a judgment without reading has gripped the entire field very tightly. I can only hope that when the reviews become open, readers will stop confusing between peer review and validation. Reader will stop relying on the blind faith that reviewers have done a good job and what they read now is reliable and true. Instead, readers would use their own judgment aided by the peer comments and as a result the reading culture will have to improve. If the entire community continues to make some quick judgments only based on the name of the journal, at the most reads only the title and abstract and feels no need to read further, then only God can save science.
Many years ago, just past my mid career, someone asked me, “When do you think was your best time in academia?” I replied in less than a second, “I think, my best is yet to come”. We talked further on this. The belief behind her question was that in any creative person’s life there is a relatively short period of very high creativity or valuable output. It might be just a stroke of luck or perhaps that much creativity cannot be sustained lifelong. There are many examples of this in the history of science as well as arts, she said.
I do not know whether this is generally true or not, but if I ask the same question to myself, my answer would still be the same even after retirement. My best is yet to come. What I mean “best” here is in terms of understanding, creativity, disruptive thinking, innovativeness, curiosity and productivity in science. I can actually feel it growing rapidly after retirement, despite many limitations such as no funding, few students around to work with, some inevitable loneliness in work and so on. Perhaps even more serious limitation, in the view of those who believe in it, would be that I won’t be able to publish anymore in journals having unreasonable author charges as I have no money to pay.
What is getting better and why? First of all, any academic rituals such as PhD no more interfere in my research. The invisible peer pressure which restricts your direction of thinking is no more felt. No career worries exist for me or for any one working with me. After being free of academia, my output actually increased instead of decreasing. Not only in terms of the number of papers but also the diversity of problems addressed, the depth of work (if not the volume), the challenges posed to prevalent beliefs, the cleanliness of arguments and so on. Out of my lifetime work, if I rank the quality of my own papers, many of the topmost came during the last five years after having quit academia. So at least in my experience, academia created more hurdles in my path than helping out. The only true help of academia was of course the salary received. It was so much in excess of my needs that it let me save and invest in such a way that now I can continue to work without any salary. At times even support a needy student from my pocket.
My perspective of science is encompassing new dimensions that we never learnt as students and ignored as researchers. Science is not only about questions, hypotheses, experiments, data, analyses, inferences and all. It is fundamentally a highly complex and continually evolving behavioral and social process that cannot be separated from the core principles of science. In fact visualizing the principles of science independent of the behavioral and social dynamics is in itself incomplete and flawed. Even in behavioral sciences training this is seldom discussed. Academia is the biggest challenge to behavioral science. This thought is not entirely new. Behavioral scientists have looked at and continue to study the knowledge process. But the angles covered so far are too few and narrow. Much of the complexity remains unexplored. I think I can visualize some of these unexplored angles better now and will keep on studying those in depth.
There are so many missing elements in the methods of science as well. People continue to work with several flaws in experimental designs and the flaws are never pointed out. The logic behind establishing a cause effect relationship is still too primitive and has many unexplored principles. At times the principles have been stated somewhere sometime but most experimenters are unaware of them. As I realize more and more of this, my understanding of science gets deeper and I wonder why nobody taught us these things in science curricula or during the research training?
I am also realizing how history, not only of science but that of economics and politics as well affects the research approach and methodologies. Science historians have not used the present enough to study history. History of the present is a big and unexplored field that reveals so much of the subtle social behavioral processes in research. Again owing to historical and ideological reasons meta-science or the science of science has locked itself in a narrow vision that it is missing a lot. I think I can see at least some of the missing stuff clearly.
I never saw the field of science with as much clarity as I have now and it is only increasing day by day, going much beyond what we were made to believe, revealing the naked realties. This should result into visualizing better design for academia. I know that nobody will listen to me, and I also know who will resist any change in academia and why. But human behavior compatible sound systems of knowledge generation and education need to be designed and only someone thinking about behavior needs to take the initiative. Everyone knows that the growing research misconduct, data fabrication, paper mills, biased peer reviews, extorting system of science publication, unscientific selection and evaluation systems all arise from bad design of academic structure. You cannot blame someone, punish someone and expect that it will stop. The academic systems need a complete revamp. But how the structure should ideally (not ideologically) be, no one is even talking about. This is the question which has become a priority investigation for me.
I do not know whether anything I study and write will be of any use to the world, but I am sure my science vision will get deeper, clearer and more useful at least to me day by day. In this sense my best is indeed yet to come!!
“I realize that in effect, I have done a lot of harm to science.”
I am personally responsible for arresting or at least creating hurdles in the progress of multiple fields of science and I proudly take the blame on myself. Any curious person working outside the temples of greater gods of science can easily put hurdles in the path of research and all he/she has to do for this is to do good research. Good research by a lesser scientist stops the progress of science.
Sounds strange? Yes, it is weird, but the weirdness comes from the weird structure of academia; especially the career paths. As I have said many times, doing good science and doing a successful career in science are two independent things, not correlated too well. In fact there are certain trade-offs between the two. You need to compromise on at least a few aspects of science if you want to build a great career in the present day academia. The way the career path creates hurdles in science is not difficult to perceive, but is generally not realized and not said explicitly.
What motivates a young researcher to investigate a certain field? It should ideally be curiosity, a troublesome question, a serious problem faced by the society and the like. The factors that actually decide what a career minded researcher decides to work on are: good chances of getting results, the potential to publish in good journals, the possibility of being the first in discovering or achieving something etc. The two might overlap at times but more commonly stand in contrast and in conflict as well.
On the other hand are the biases in peer reviews and the journal prestige. Young researchers in more reputed institutions have better chances of publishing in high ranking journals provided they meet certain criteria. They tend to chose what to work on based on the chances of fulfilling these criteria. Any replication of a new result is important for science but is unlikely to give a high impact paper. Replicating experiments does not improve career prospects. Therefore testing the reproducibility of any experiment is not the preferred line of work by ambitious researchers. The entire reproducibility crisis is because of this factor.
In contrast, novel concepts or path breaking research is not expected from children of the lesser god. Even if they do so, they can’t publish in prestigious journals since the most likely fate is desk rejection by only looking at the name of the country, university or institution. They are most likely to end up publishing in low prestige journals. As a result their work is hardly read and cited by anyone, citing a paper from a lesser journal is below dignity for the elite researchers.
So what happens when someone from an obscure background publishes a real break-through or opens up potentially a new line of work?
It is simple. That line of work will never progress. There are three ways in which this new line could have progressed. One is that the person gets sufficient funding to further the work he/she pioneered. Second could be that someone from the elite class recognizes the importance of the concept and takes an initiative to collaborate. The third, someone from the elite class develops the same thinking independently and takes it ahead with or without giving due credit to the third world scientist. In the last case there might be injustice to the third world scientist but science does progress. Even in the second case the elite may carry forward the work without collaborating or giving credit to the original discoverer. This again is unfair but science would progress nevertheless. That’s not so bad in my view. There are multiple examples of this in the history of science.
In today’s world of rapid literature accessibility, none of this is very likely. The poor original discoverer will not get funded because the concept does not come from the elite. Their work will not be taken seriously in the field since it is published in a lesser journal. Even if an elite researcher thinks of the idea independently, is excited by it and is convinced that this can bring in revolution, but discovers that someone has published it already, will not take it forward because that will not give a big career boost to him/her. The net result is that all the three paths of progress are blocked and this line of work gets arrested in spite of its potential in giving revolutionary insights.
This is what happened to my science throughout my life. I was not career conscious, but merely fond of ideas. I pursued a number of novel ideas in diversity of fields, showed their mathematical and logical soundness, supported them with evidence, primary experiments, secondary data, made testable predictions some of which accidently got tested and found support. Some of them have the potential to give a complete new turn to the field, open up new lines of thinking. But nothing of this happened or is likely to happen in near future. Nobody found any flaws in my arguments, nobody doubted their validity and relevance to the field, I came to know that some giants in the field were quite aware of what I published and appreciated it in private. Still nothing happened further on these lines. I never got funded to continue work on my own idea. (I did get huge funding at times but that was only when I towed the line of a giant in the field.) I could not publish my original ideas in the top ranking journals because they were declined every time without review. Some of the ideas were very obvious but just a little ahead of time. So I can’t believe that no one else thought of these any time independently. But once I published first, there was no body interested in them.
I realize that in effect, I have done a lot of harm to science. Anyone working outside the mainstream community and doing good science actually creates hurdles in the progress of science. Whom shall we blame for these hurdles? It seems to be a crime to do creative research, generate novel and sound ideas outside the main stream and someone like me is a criminal in the field.
Transparency of methods, data, analytical tools, programs used is extremely important for science. This is well recognized and many journals ask many questions to authors to ensure transparency even before processing a manuscript. Ironically peer reviews, which form the backbone of today’s science publishing, are not transparent and accessible to anyone. I haven’t seen a bigger contradiction in my life.
Recently I uploaded two papers on the open peer review journal Qeios. One titled “Behavioural optimization in scientific publishing (https://doi.org/10.32388/8W10ND.3)” and another more recently uploaded “Evolution of new variants during the SARS-Cov-2 pandemic: mutation limited or selection limited? (https://doi.org/10.32388/LLA6AO)”. The first one, in less than one month has received 13 reviews (in addition two elaborate responses to me on email) and has undergone two revisions. This response is unique in my experience, both in terms of promptness as well as rigor. The most common scenario with conventional journals is that most reviewers respond only after multiple reminders. It is obvious that many of them have not read the complete manuscript. They would raise questions which are elaborately answered already in the paper, would make sweeping statements without giving a single reference, or suggest citing references that are not relevant. In contrast, this paper received both appreciation and detailed critical comments. Differences of opinion were expressed without hesitation, but there were no derogatory remarks that I have seen so commonly in confidential peer reviews.
I spent a total 7-8 full days in reading, preparing detailed responses and revising twice, which I fully enjoyed. With one person I had an online discussion as well. Numbers are not enough to reveal the real fun of open peer review. The mindsets during the interactions were unique. In conventional peer reviews, while the authors are revising or replying to comments, scientifically sound arguments are not enough. They have to worry about satisfying the reviewer along with his preconceived notions, prejudices and egos. There is no choice but to please the reviewers. I have experienced this from both the ends and have written about it earlier (https://milindwatve.in/2020/09/17/how-peer-reviews-are-degrading-the-spirit-of-science/). This time I found myself only committed to logical soundness of arguments without worrying about the interpersonal complexities. Wherever we differed I had no hesitation saying that we differ on this issue. I had the same feel about the interacting reviewers too. This is great. This is a real platform for science.
This anecdote strengthens my notion that open peer reviews will improve the quality of reviews substantially. There has been a debate about open peer reviews multiple times on different platforms. Many people fear that this will increase the responsibility of reviewers and therefore they will be even more reluctant to review. We already have dearth of reviewers. Does 13 reviews and 2 revisions within one month support this fear? There were worries expressed that reviews will not be critical enough. Just read the reviews to this paper to see whether that is true, they are all there for everyone to read on the same link.
The most important point is that anything that is not transparent is NOT science. I have over 200 experiences of receiving peer reviews, dozens, if not hundreds of peer reviewing for journals until I started replying to review requests that I will accept only if you make it public. This is not a small sample size. I received high appreciation as well as irresponsible and insulting remarks, highly entertaining stupidity and “oh, how come I didn’t think of this” feeling. But still I would say this is the first time in my life I thought I was doing science and only science. On all previous occasions there was a feeling of either facing an exam or standing in the court of law. The word “peer” indicates standing on level grounds. First time in my life I was really standing on level grounds and talking only of science. In this sense this is the first “peer” review of my life. All others felt like being a criminal under trial. My sincere request to all fellow researchers to experience this, from both the ends, as authors and as reviewers. Open peer review is the future of science, if science has to be science all the time. Otherwise the flaws, biases, power play, inequality, racism, discrimination, regional imbalance, exploitation, bad incentives, reproducibility crisis, research misconduct which is evidently growing in the field will end up with the entire field harboring only pseudoscience.
I know that open peer review journals will have tough time for quite a few years owing to the religious and aristocratic social structure of the scientific community. Right now the community is deep in a pit of the illusion of journal prestige and CV building. The culture of evaluating one’s research without reading it has created a trap for everyone. Anyone with career worries will not be able to do open science for the fear that any attempt to do so will ruin my career. I must only try to publish in high impact journals. This cowardice will prevent science from being science for a long time, but I am an optimist. Science will certainly become true science some day.
When a team of researchers is employed by an agency such as an institute or a company, and they find something worth publishing or patenting, whose intellectual property is it?
By the norms followed the world over, it is the property of the agency by default. Other types of understandings are off course possible but that needs to be clarified in the employment contract or the appointment letters. If not, the agency has the right to decide the norms by which credits and any other benefits coming from the intellectual property can be shared and distributed among individuals participating in research. Generally this goes well.
But there is an unusually complex situation in Indian academia. Quite often the fellowships or salaries of the students, project assistants, laboratory assistants and other project related staff are not paid for quite a long time. This can range from a few months to sometimes 2-3 years. The causes for this lie in the inefficient and careless handling of the funding and related paper work by the funding agency and the research organization equally. Interestingly the salaries of faculty, administration and other permanent personnel are almost never delayed. Often the funding agencies and the handling machinery is the same. But they are more careful about the permanently employed people and utmost careless about students and project staff. The reasons of course lie in the nuisance value. Permanent government employees have a history and tradition of having strong associations having fought for their rights and pay-scales. Students and short term project staff are the most unorganized sector workers and therefore get helplessly exploited in a number of ways and the higher ups in academia do not care to improve the situation.
However, the intellectual property angle of this problem remains unappreciated. The institutes hold the rights on intellectual property because they pay their employees regularly. But if that is not happening, the standard IPR norm collapses. Individuals who work without the promised pay can claim the first right on all the intellectual property generated during the time period of their work. The institute cannot claim it because it has not paid. Even if there is any kind of employment contract, failure to pay the salary in time is the breach of contract. If an agency is responsible for the breach of the contract, its right to claim any other benefits from the contract comes under question. The faculty, PIs of the project are getting their salaries regularly, so they cannot claim the IPR. Under such circumstances, the unpaid workers have the first right on IPRs. The institute cannot publish or patent the work or even include it in any of its official reports without the written permission of the unpaid workers. Research is a complex task and it is difficult to decide who contributed what. Often the persons actually doing the work know the subtleties of an experiment much better than their guides happily occupying their easy-chairs. Therefore the norms of IPR sharing need to be pre-decided. Violating these norms would potentially lead to unprecedented legal complications.
The simplest way to avoid any such complications is to pay all research personnel their due amounts in time. The reason this does not happen is lack of motivation to set the system right. There is no other reason that the funding system cannot correct itself. But as long as the institute does not lose anything by being careless, nobody will try to remove the system flaws. Therefore it is necessary that there are at least a few cases whether the unpaid researchers claim rights over the intellectual property and prevent the institute from using any of the research output.
The reason this has not happened so far is twofold. One is that this interpretation of the IPR norms is not known to anyone although logically it is quite straightforward. But even more important is that the sufferers do not have the muscle to challenge the system. They are in an insecure position and fear that the higher ups control all their career prospects. The academia is completely aristocratic in multiple ways. So most sufferers will not dare take any bluntly logical stand. But it is not impossible. I can imagine that someone has to leave when a project ends and there is no hope of continuing. For a person in such a position, there is no risk of losing anything anymore and such a person can block the entire output of the project that he/she was working and prevent the institute from using it in any way. Institutions and funding agencies need to be aware of this interpretation of the IPR law and correct the system in time without any excuse. If that doesn’t happen, the junior research personnel should come out and act. If not in the court of law, then they can come out in the public domain. Let people be aware of the reality. Let common man start asking questions to Directors, Chairs, Heads and PIs, “How many unpaid researchers work under you?” A whip from common man can be the ultimate motivator.
Recently I had an experience of an open peer review journal and it is certainly worth sharing.
As a student of behavior I have been thinking of the behavior of different players in the science publishing system and whether we can design a behaviorally sound system that would minimize biases , misconducts and irresponsible behaviors in the peer review system. I gave a talk on this in December 2017 and a preprint article in 2019. Interestingly in 2019 itself an open peer review journal called Qeios (pronounced like chaos) was started on very parallel (but not quite the same, some crucial components from my system missing) principles. Qeios started as a preprint repository but also has a peer reviewed publication system but with no dichotomous editorial decision involved. An AI system searches for and invites reviewers. Reviewers are informed that their reviews will be public. Authors can respond to them, improve their paper if needed but all these steps and stages will be completely transparent.
Any new journal has initial problems which this journal will also have for quite some time. Because of the impact factor illusion and the sheep mentality of researchers, a new journal is unlikely to get high quality papers in the initial years, which seems to be true for Qeios as expected. When I received a review request, I didn’t expect a high quality paper. What I received was not bad, it had some thought provoking ideas, but the work was not rigorous enough, being sort of aimless and not contributing any new and meaningful insights. At the same time it was Ok in terms of the model developed and some of the data and discussion.
Although I have been advocating open peer reviews for many years now, while preparing myself for an open peer review I realized something that I had failed to appreciate before. For a conventional journal I would have recommended rejection. I realized that it would have been a very dumb and non-productive end. The paper certainly had triggered some thinking in me. I thought of some new questions, some ideas, some tricky issues for the first time. It was not enough to make a full paper in itself, but it was worth something. If I expressed my doubts, my half baked ideas it would possibly stimulate someone else to think. They may have solutions that I couldn’t think of, or they might simply add more questions, may even point out that I was wrong. All this is a valuable process, not a product. But so far we were only publishing products and hiding the process. That is only half science. Open peer review journals can bring out at least part of the thinking process and much can be learnt from that. May be at a later stage I will return to my own arguments and develop them further. May be someone else does so. If I had recommended rejection, then nothing of this sort would have happened. Me too would have forgotten the issue in no time. Publishing the thinking process enriched me substantially. Of course not everyone will do this. There would be a lot of junk published. It is true that some people would only write goody -goody reviews and since it is published, add to their CV. This is happening. That might be inevitable garbage, but not a sufficient reason to block the valuable open thinking process. Here is the link to what I wrote as a reviewer (https://www.qeios.com/read/S390H3). The author responded to my comments, not with much rigor but that’s ok. Everyone has limitations. If it is in the open domain someone else can compensate for these limitations sometime and take the concept to a meaningful level. I hope people understand and realize the strengths of open peer review and adopt this practice increasingly. The starting problem of quality would vanish eventually.
If simulating modal human thinking is the goal of artificial intelligence then I would certify chatGPT is highly successful. It is as stupid as humans except that its stupidity comes much faster.
Having taken interviews, oral examinations, PhD or master’s thesis defense over a long time, I have been often struck by a class of students who talk a lot and give a lot of information without even touching the answer to the pointed question asked. Sometimes, and not rarely, they get away making a good impression. My interaction with chatGPT reminded me of such students.
I started exploring chatGPT after having postponed it for a long time. I thought AI would be better than humans in areas in which computers are obviously more efficient. That is in compiling large data, using quantitative methods, verifying an opinion against published evidence etc. But it doesn’t do anything like this. It doesn’t claim to do such things. It only repeats what has been said more often and by the elite, irrespective of whether it is true or not, logical or not, self contradicting or not.
I was particularly keen to see what it does when there is a contradiction between the belief in a field of science and actual data. So for obvious reasons I asked questions about diabetes. It started answering with the typical mainstream belief. When I pointed out that there was evidence going against it, it admitted that there is, but again started reiterating the beliefs. Then I pointed out that your statements are mutually contradicting, on which it admitted that there are contradictions and gave an excuse that the system is complex. When I gave specific evidence that shows his belief was wrong, he said yes there is evidence on the contrary but again went back to the belief. When I questioned what the evidence for this belief is, it said there is plenty of evidence from decades of research without giving any specific experiments or data as evidence. You can access the entire communication here (https://drive.google.com/file/d/1IhiFoscOWwD_cxhGguO0ssd7tkwmyiiW/view?usp=sharing).
This is precisely what people in this field have been doing. Everyone knows that multiple lines of evidence directly contradict the theory but they are not willing to give it up. They continue to live with circular logic, falsified hypotheses, internal contradictions and complete clinical failure but they will still continue with it, keep on cherry picking convenient findings and claim that they are doing science. It looks like AI is also an expert in this kind of self deception. This is fine, if your definition of intelligence itself is mimicking human thinking. But there is one important component missing. Human behavior has huge individual variability. While for modal personalities conformity is more important than logical soundness, there is a rare individual who craves for sound logic, someone who looks at data more than opinions. Science progresses by such outliers, and not by modal human thinking. If AI is like modal human intelligence and does not incorporate the outliers, it would prove to be retrogressive rather than progressive. People have already started using chatGPT in research. There are talks about AI doing peer reviews and all. Even if such a use of AI is officially banned, people are going to use it I have no doubt. This is the greatest risk. Using this kind of AI in science will only increase the conformity bias and make publishing disruptive thinking, surprising results, path breaking and paradigm shifting research increasingly more difficult.
One more step in my commitment to transparency in peer reviews
The dictionary meaning of “peer” is “a person who is of the same age or position in society as you.”
This meaning of peer is expected in peer reviews. Peer reviewers are not like “examiners” of a student candidate. They are supposed to be at the same level of scientific standing as the authors. Therefore the norms and responsibilities of science writing that are expected from the authors should be applicable for the peer reviewers too. For example, author of a scientific paper is expected to support every important statement by either citing reference from prior studies or by his/her own logic and evidence. The same rule should apply to a peer reviewer. But rather too often it is seen that peer reviewers make sweeping statements without even a minimal attempt to support them. More alarming is the fact that editors have no hesitation in accepting it simply because it comes from a reviewer and not from the author. With such double standards this cannot be called “peer review” by definition. The minimum standards applicable to authors should be applicable to reviewers as well and editors do not have the right to give differential treatments to authors and reviewers.
But reviewers make irresponsible comments quite often and get away with it because peer reviews remain confidential. Editors cannot reject a review because reviewers have become a rare commodity. Hardly anyone is willing to “waste” their time in reviewing others’ work for which they get no credit. If editors insist on higher standards from reviewers, getting manuscripts reviewed will become orders of magnitude more difficult. Therefore they are compelled to compromise on the quality of reviews. As a result, the review quality is degrading rapidly and nobody cares because they remain confidential.
I am copying below the correspondence that I recently had with the journal “Evolution”. Let me state very clearly that Evolution is a very respectable journal and I have no intention to single out this journal for criticism. I completely respect the editors, some of them being good friends of mine. But all journals suffer the same ailment. I just happen to have a fresh example from this journal, therefore I am making this correspondence public.
I am sure that the editors won’t like this. I may convert my friends into not so much of friends. It is just too natural if this act affects my chances of getting papers accepted henceforth. I also consider the possibility that the journal takes any kind of action on me officially. But that’s ok. I am doing this as a part of my commitment to transparency of peer reviews. If only a handful of authors start making the reviews public on their own, the review process will become more responsible in no time. But any researcher who has to worry about his/her career will not be able to do this. I can afford to do this because I don’t have any career. So I can keep the broader interest of science above career concerns.
Earlier with the same journal, I received a review request and I wrote back that I am ready to review if the journal agrees to make the review transparent. They did not agree and therefore I declined to review. My commitment is therefore independent of my position. I did not raise the issue because my paper was rejected.
I am pasting the entire correspondence of both the incidences with the journal Evolution below for the readers to evaluate and interpret themselves. Improving the quality of peer reviews is just too important to keep it under the rug.
13-Feb-2023 Dear Dr. Watve:
Thank you for submitting your manuscript, “Evolution of new variants of SARS-COV-2 during the pandemic: mutation limited or selection limited?” (22-0518) to Evolution. It has been evaluated by Associate Editor Dr. Maria E. Orive and two reviewers, whose comments are appended below. Unfortunately, these evaluations, as well as my own appraisal, indicate that your manuscript is not suitable for publication in Evolution.
I am sorry that the review process took so long. Although I realize you will be disappointed by this decision, I hope that you find the feedback useful for considering submission elsewhere or for planned future directions with the work.
We appreciate your interest in publishing in Evolution and hope that this decision will not discourage you from future submissions.
Associate Editor Comments to the Author: Reviewer 1 points out some very important issues with the approach taken by the analyses in this manuscript; the information known about the spread of variants of SARS-CoV-2 show that conditions given by the approach distinguishing between the hypotheses of selection versus mutation as the limiting factor for spread are not correct for such novel infectious diseases. As such, the approach taken appears to be fundamentally flawed.
Reviewer(s)’ Comments to Author: Reviewer: 1
Comments to the Author I do not think this paper is suitable for publication. Unless I have misunderstood something it puts forward a rather naïve approach for distinguishing between selection versus mutation being the limiting factor in the spread of variants of SARS-CoV-2, and it then uses this approach to infer from data that selection has been the primary limiting factor. This, despite the fact that we know this is probably not the case for all major variants that have spread, up to and including Omicron. Thus, to my reading the ms uses an approach that almost certainly can’t work for the data at hand to conclude something from the data that we know is almost certainly not true.
The problem with the approach is at least two-fold. First, the main focus of the approach assumes that immune-mediated selection is the primary selective factor but we know for novel host-pathogen associations like SARS-CoV-2 and humans, that the most important selective factor initially will be differences between humans and the ancestral host. When one incorporates that into a model one sees that the first several variants that spread will tend to be driven by strong selection for adaption to the new host, irrespective of immunity. So the conditions given for distinguishing between the hypotheses are not correct for such novel infectious diseases. And we know this is important in SARS-CoV-2 because Alpha and Delta (and probably Omicron) were all selectively advantageous regardless of the immune status of people in the populations. Second, the goal also seems to be to use the appearance of waves of infection in COVID as a potential signal of the underlying evolution but we know that this was not the case for many (perhaps most) waves for the first year or two. Instead, waves were almost entirely driven by changes in behavior mediated by public health measures and seasonality.
The problem with the conclusion of the ms is that we know for Alpha, Delta, and Omicron that selection was not the limiting factor. As mentioned above these variants were unconditionally advantageous, regardless of immune status. Further, the spread of these variants in a location was entirely migration limited. Each of them appeared in different geographic locations (England, India, South Africa) and then spread through migration to other countries. It was only once these variants arrived through migration that they increased locally, and they did so somewhat independently is different countries despite the countries having very different immunological histories. On top of that, each of these variants had a very unusual constellation of a large number of mutations, further arguing that mutational appearance was the most important limiting factor.
Incidentally, if one wanted to determine the role of selection versus mutation in the spread of variants then why not look at the phylogeographic data? If the process is mutation limited then won’t Delta variants across the globe, for example, have a common Delta ancestor? If instead selection is the limiting factor then, for example, Delta should spread at different times in different populations depending on their immune history, and they should not share a common Delta ancestor.
Other comments
P2 – migration should also be mentioned and included as an important evolutionary factor, particularly for SARS-CoV-2.
P3 – I think the characterization of models that incorporate immunity is unfair here. There is a very large literature on this. Furthermore, immunity can be binary and still display gradual loss of immunity at the population level (which is probably what matters here).
I also think that, throughout the ms, there is a tendency to conflate the issue of the spread of a variant with the occurrence of a wave of infection. These are distinctly different things. For example, in many locations, when Alpha was initially increasing in frequency, the overall number of infections was decreasing (which is why many authorities were hesitant to impose lockdowns initially).
Reviewer: 2
Comments to the Author All the arguments made here are sound but they are not in the least novel. The authors have ignored 30 years of work in strain dynamics to start from scratch in understanding a very basic feature of the emergence of novel variants within a standard epidemiological framework which applies to SARS-CoV-2. They conclude, correctly, that the new waves are not likely to be “driven” by the emergence of variants – but, I’m afraid to say, that is a result that has been in the literature for at least 30 years.
14th Feb 2023
Dear Dr. Mirium,
Thanks for your letter of rejection and comments by two referees. Rejection is an inevitable part of the publication game and we take it in a positive spirit. Simultaneously we have some queries for which we would like to seek answers and clarity about the editorial policy of Evolution.
1. What is the meaning of “peer” by your norms? By dictionary meaning, peer is at the same level of social or organizational status. Therefore the set of norms for authors and peers should be comparable. If authors are expected to support every statement by citing appropriate reference or with new evidence, aren’t peers also expected to do the same? Both the reviewers of our paper make many sweeping statements neither citing relevant literature not giving any evidence. If authors’ manuscripts can be rejected because of inadequate evidence, do the editors have a policy to reject reviewer’s comments based on the same set of norms? How frequently in the last few years the editors of your journal have rejected reviews if they do not comply with the same norm as authors?
2. Reviewer 1 says multiple times that “We know that this is not the case…..” “We know that ….selection was not the limiting factor” and so on but does not indicate the data on the basis of which we “know”. In the absence of any supporting rigorous study cited, this can be at the best taken as the reviewer’s belief. We independently searched but did not find any rigorous study supporting the reviewer’s multiple beliefs. If it is a case of belief versus evidence, does your journal go by belief or by evidence? Let us clearly know the journal norms.
3. The two reviewers starkly contradict each other. Reviewer 1 says that our arguments are not sound and reviewer 2 says that they are sound but not new, that is, they are already well established. This clearly shows the irreproducibility of peer reviews. Does the journal think that in order to increase reproducibility of science, first there needs to be a minimum level of reproducibility in peer reviews?
Kindly understand that we are not challenging the rejection or appealing a reconsideration. We accept the discretion of the editor. We are only seeking some clarity about the journal’s general norms on which manuscripts are accepted or rejected. In the broader interest of science it is necessary to ensure that the norms follow the minimum necessary principles of science.
One more earnest request: We believe in transparency of peer reviews. Since the manuscript is on preprints archive, we would also like the peer review reports and our response to it respectfully posted on it. We would like to have your consent to post the peer reviews on the preprint server or any other appropriate public domain. It would also be in the interest of science that this correspondence is made public appropriately and respectfully. Transparency is the first requirement of science and I believe you will not disagree. So kindly let us have a written consent to make the entire editorial process for this manuscript public.
Thanking you and awaiting your response eagerly.
milind
Miriam Zelditch
Tue, Feb 14, 9:03 PM
to Tracey, me
I am forwarding your message to the Editor-in-Chief of Evolution.
—
Miriam Zelditch
Tracey Chapman (BIO – Staff)
Feb 23, 2023, 5:24 PM (7 days ago)
to managingeditor@evolutionsociety.org, me, Miriam
Decision on Manuscript ID 22-0518
Dear Milind,
Thank you for writing with your concerns and queries, which we have considered carefully. I also took a fresh look at your MS, the reviews and decision-making process. You raise three inter-related points: (i) assessment norms for authors vs reviewers; (ii) third party support for reviewer assertions; (iii) contrasting reviewer reports.
The reviewers of your MS gave different perspectives and contrasting reasons and assertions in their assessments. This is not unusual, and editors are trained to integrate sometimes disparate views, which, as in this case, may have varying levels of depth. They pick out the substantive, evidenced concerns, and down-weight others in order to come to a recommendation and then decision. Editors don’t ‘vote count’ but integrate the information according to professional standards https://academic.oup.com/pages/authoring/journals/preparing_your_manuscript/ethics?login=true#peer. We always aim to make it clear which are the key elements that feed into the final decision (though as reviews are supplied verbatim, that may not always be so apparent from an author’s perspective).
You are not challenging the decision on your MS, so I don’t comment in depth on any specifics. However, my assessment is that some substantive and legitimate concerns were raised by the first reviewer. For example, they described in some detail their concern, supported by observations, that the approach used could not distinguish between selection vs mutation. The expert AE comments specifically on this main point of concern to justify their decision and I agree with this assessment. The second review, written in somewhat stark terms I agree, was not central to the final decision (had the outcome had been different, we would have asked you to counter it). Overall, I find no concerns with the quality of decision-making rendered on your MS.
You also ask that we consent to make the entire editorial process for this manuscript public. This journal uses double-anonymised peer review, rather than a fully open peer review process, to minimise the influence of well-known unconscious biases on decision making (e.g. Ware et al. Info Serv & Use 28 (2008) 109–112). As part of this process, reviewers are informed that all communications regarding the manuscript are privileged, so sharing their reviews without their permission would raise potential ethics concerns. Therefore, we ask that you respect this confidentiality if you can.
Thank you again for raising your concerns, which we do appreciate,
Best wishes,
Tracey
Prof Tracey Chapman | School of Biological Sciences
Editor in Chief, Evolution
Milind Watve<milindwatve@gmail.com>
Feb 24, 2023, 9:30 AM (6 days ago)
to Tracey, Miriam, managingeditor@evolutionsociety.org
Thanks for your valuable response.
Since, as you agree and as so many studies unanimously demonstrate, the peer review process is inherently and seriously biased, any debate regarding the fundamentals of the process are most welcome and in fact badly needed.
I had asked three questions and you appear to have not replied to two of them.
I asked whether there are different standards for authors and reviewers by your journal norms. For example the authors are expected to support every statement they make, but reviewers are allowed to make sweeping statements without support. The answer to this question could only be yes or no. No other wording can be an appropriate answer. I also asked if there is a situation of belief versus evidence, what do your journal norms go by? I also did not find any answer to this.
Whether rejection to our paper is justified or not was not the question at all, and you have answered the unasked question quite elaborately.
I thank you for answering the third question that if the two referees contradict each other, the editors use their own discretion. In this you have also clarified what I asked. Editors do reject some of the reviews. The further natural question is whether the reviewers are conveyed your rejection as you do it for authors? If not, again do your journal norms permit different standards for authors and reviewers. It’s ok if the answer is “yes”. Only clarity and transparency in the norms is what I request.
I beg to differ with the last point. Double blind reviews are psychologically impossible. The moment a reviewer sees a manuscript his/her mind immediately starts guessing who it could be. This is human nature and can’t be surpassed. I have worked as a reviewer multiple times and asked so many other reviewers as well. In small fields it is frequently possible to guess. Further, preprint practice directly contradicts and nullifies the attempt to conceal the identity of authors. Since preprint is a well accepted practice, double blind peer review remains only a pretense. Transparent peer reviews is the only option that will improve the peer review process.
Since I am a strong promoter and supporter of transparent peer reviews, I am afraid I will make all attempts to make this correspondence public. I am a small man and nobody would notice it. But I have to remain honest to my principles. The journal is welcome to take any legal action against me if necessary.
I will also continue to communicate manuscripts to your journal, and if you decide to reject them on the grounds that I don’t agree with the confidentiality norms, kindly reject them clearly stating this reason.
My thousand apologies for all the trouble, but this is a necessary trouble in the broader interest of science.
The darkness on the path to truth is my homeground. If the dazzling lights in the rest of the world are under your command, why should I care!!
Earlier correspondence related to me declining to review for the lack of transparency
Evolution<onbehalfof@manuscriptcentral.com>
Thu, Dec 8, 2022, 11:10 AM
to milind.watve
08-Dec-2022
Dear Dr. Watve:
Thank you for replying to my invitation to review for Evolution.
It is unfortunate that you are unable to review this manuscript at this time. I will keep you in mind when future manuscripts come in that fall under your area of expertise.
If you have a suggestion for an alternate reviewer and did not provide this on the site, please email the editorial office at managingeditor@evolutionsociety.org with your suggestion. Please also include the manuscript number EVO-22-0577.
Sincerely,
Dr. N. G. Prasad Associate Editor, Evolution
Dear Prasad,
I wrote the following to the managing editor address.
Dear Editor,
I received a request to review a manuscript from your journal.
I am declining for the following reasons.
After being grossly disappointed with mainstream science, I have been working with undergraduate students, farmers, tribes and other people doing real and truely enjoyable science. While doing so I feel the hypocrisy of mainstream science even more. Thinking over a few years I have reached certain decisions.
I have been fighting for transparent peer reviews for quite a few years now. As an author, I am at the receiving end and can do little about the system. But whenever requested to be on the other side of the table, now I will demand a change in system. I will do reviewer or guest editorial jobs only if the journal is ready to make the entire process transparent. What I mean is that all reviews, comments and decisions are made public by appending them to the preprint on a public access server. This should be independent of acceptance rejection. With the opaque and therefore dubious peer review system, I think I should not waste my time because as it is peer reviews do no good to science.
I request your journal to rethink about the peer review system. If that happens I will give my 100% to it. If not, kindly do not request my inputs for any manuscript hereafter.
After quite a few years I attended a conference, ISEB4, the 4th meeting of the Indian Society for Evolutionary Biology in Ahmadabad last week. It was a refreshing experience particularly watching the younger generation of evolutionary biologists coming up. Also promising were the new centers of evolutionary biology and ecology coming up at different Universities and Institutions in India.
But simultaneously I could hear a subtle alarm bell. Things are moving ahead, no doubt, but are they getting too stereotyped?
Yes, unfortunately they are. The career paths of science, the definitions of success, the paucity of positions, the necessity and the ways of building an “impressive” CV, the modalities of getting funded are all getting increasingly narrower. Bottlenecks are getting too tight and that, down the line in a just a few years would be largely counterproductive. We see that most youngsters stick to the line of work they followed in their PhD, which was a continuation of their parent lab’s already established line of work. They take a small variation of the same line as their plan of work. Following a narrow field of work for several academic generations is not detrimental to science, but doing only this and not looking beyond certainly is. Nobody ventures into something new because for recruitment or for funding they are asked to present a research plan, then they are asked what experience do you have in this, how do you know it would succeed? So only sticking to the old is safer and that works. Novel ideas fail at every stage. This peril is brought about by the stereotyped and ritualistic career paths. The antidote is that the career paths need to diversify in more than one ways.
I use the word diversify in multiple dimensions. Diversifying the field of investigation, the model organism or the model system, use of novel and diverse tools as per the need of the problem, addressing novel and entirely virgin questions, diversifying the system and including more kind of people in science; all this will only enrich science. I don’t think anybody will disagree with this. But what prevents diversification is the ritualistic career path. The system and the criteria for evaluating a researcher for recruitment, for promotions and for funding have become rigid, ritualistic and often non-sense. The minimum requirement for a faculty position is PhD, three years or more of post-doc, an impressive number of publications, at least a few of them being in flag ship journals. Do these qualifications guarantee a good candidate? The answer is no. A good CV might just be because of the luck in getting in a good lab. Does not having such a CV indicate lack of talent? Again the answer is no. But institutions look at on paper qualifications more than the talent, capacity and dedication.
My doubts about this ritualistic requirement are too fundamental. In the field of literature, everybody does not need to write a novel. Short stories and even three liner haikus bring equal respect if they are of an appealing quality. But in science, only a thesis gets you PhD and without PhD a career in research is impossible. A two page theorem can potentially revolutionize a field of science, but that cannot make a thesis and therefore cannot make a career by the current stereotype. Since people only look at the number of papers and impact factors, reading one’s research with interest has almost lost its relevance. What kind of science is published in big journals and who can publish in big journals is also more of a tactical issue than a quality issue. Getting a position and getting funded is also more tactical. Only a stereotyped format is expected in a funding proposal. I can see young researchers thinking too much about these tactics and ignoring their own natural questions, attractive curious findings, urge to explore and zeal to find something really novel. High risk disruptive ideas are most unlikely to get funded. As a result novelty, exploration, disruptive elements, rigor, insights, paradigm shifts have largely taken a back seat. Research is being sold by gallons rather than by taste and flavor. The perils of this ritualized science are increasingly coming to light in terms of scientific misconduct, reproducibility crisis, peer review biases, stress-anxiety and suicide rates among students.
Changing the mainstream is almost impossible, but that’s not what I am suggesting. My solution is to support alternative models of doing science. Why should PhD be the only path for getting into research? Why can’t housewives do meaningful and fruitful research? Why can’t farmers solve their own problems by participating into research? Why can’t Universities join hand with citizen forums to address important questions? Throughout my entire life I have experienced the alternative routes, experimented with and demonstrated that they work. The alternative models of doing research are like collaterals in heart disease which keep the heart pumping even if a main vessel is blocked.
While clear pathological signs are accumulating in mainstream science, we need to focus on development of collaterals. Who can do this? I believe the new upcoming academic models such as private Universities, autonomous colleges, liberal arts curricula, citizen science forums can do this and they need to be strengthened. If these models take pride in mimicking the mainstream again, they would simply join the mass sugar coated collapse of academia. Their real strength lies in doing what mainstream is NOT doing. Asking questions which the mainstream is not asking. Tapping new possibilities and trying out crazy ideas. Being open to failures and traverse new paths. I am trying to search for an element of such vision in these alternative models. I do see some vision in some of them and hoping it develops into a fruitful diversity of models of practicing science.
The diversity of research models will fill in the big voids that currently the mainstream science is unable to cover. Most mainstream scientists are too specialized, narrow minded and fail to visualize bigger and comprehensive pictures. Most have been generating huge amounts of data that haven’t been interpreted collectively and comprehensively. Main stream typically fails to look at alternative possibilities and interpretations which are more likely to come from non-career-minded thinkers. Owing to the rat race for high impact publishing main stream rats seldom try to test reproducibility of results. Spending time in testing reproducibility is a waste of time for them because that is unlikely to get a high impact publication. Since funding is highly biased towards a few buzz words, mainstream does not go beyond trend following. The other alternative models can do such things which are extremely valuable for science and the society. If we fail to develop these collaterals, the mainstream will continue its downfall until common people lose trust in science. Technologies and even basic science will be completely monopolized by a handful of agencies and companies (this is already happening in science publishing) and people will be completely alienated from science.